![]()
HIPEC for peritoneal cancer
-patient information-
Stefaan Mulier, M.D., Surgical Oncology, Leopold Park Clinic, Brussels, Belgium
What is peritoneal cancer?
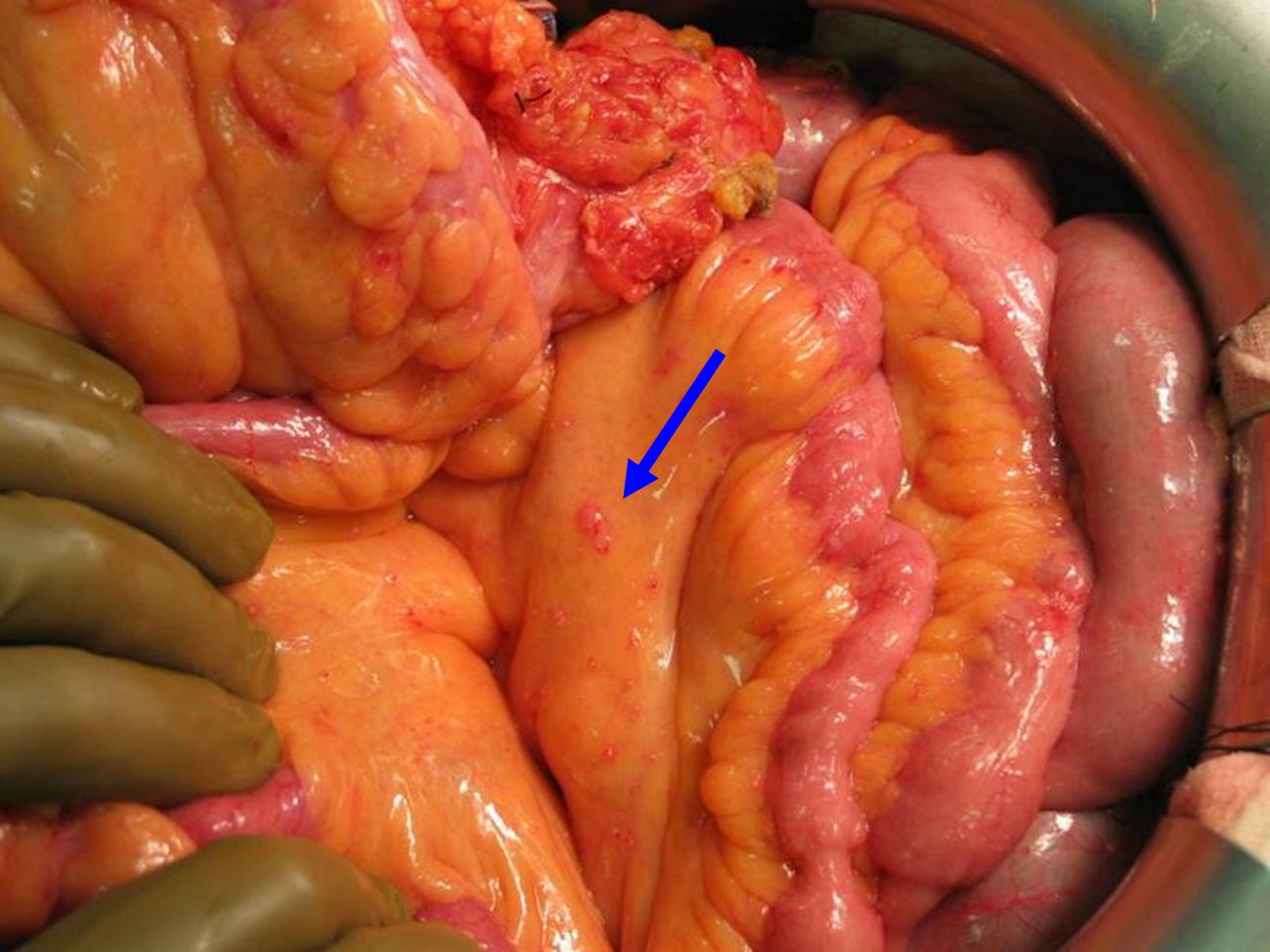
The peritoneum is a glistening membrane which covers all abdominal organs. It secretes the peritoneal fluid, which enables the bowels to move smoothly during the propagation of food. Its surface is as large as the skin surface, 2 square meters.
Peritoneal cancer means the presence of cancer cells on the peritoneum. Below you can see the small bowel, covered by the glistening peritoneum, with several small pink implants of cancer cells (blue arrow).
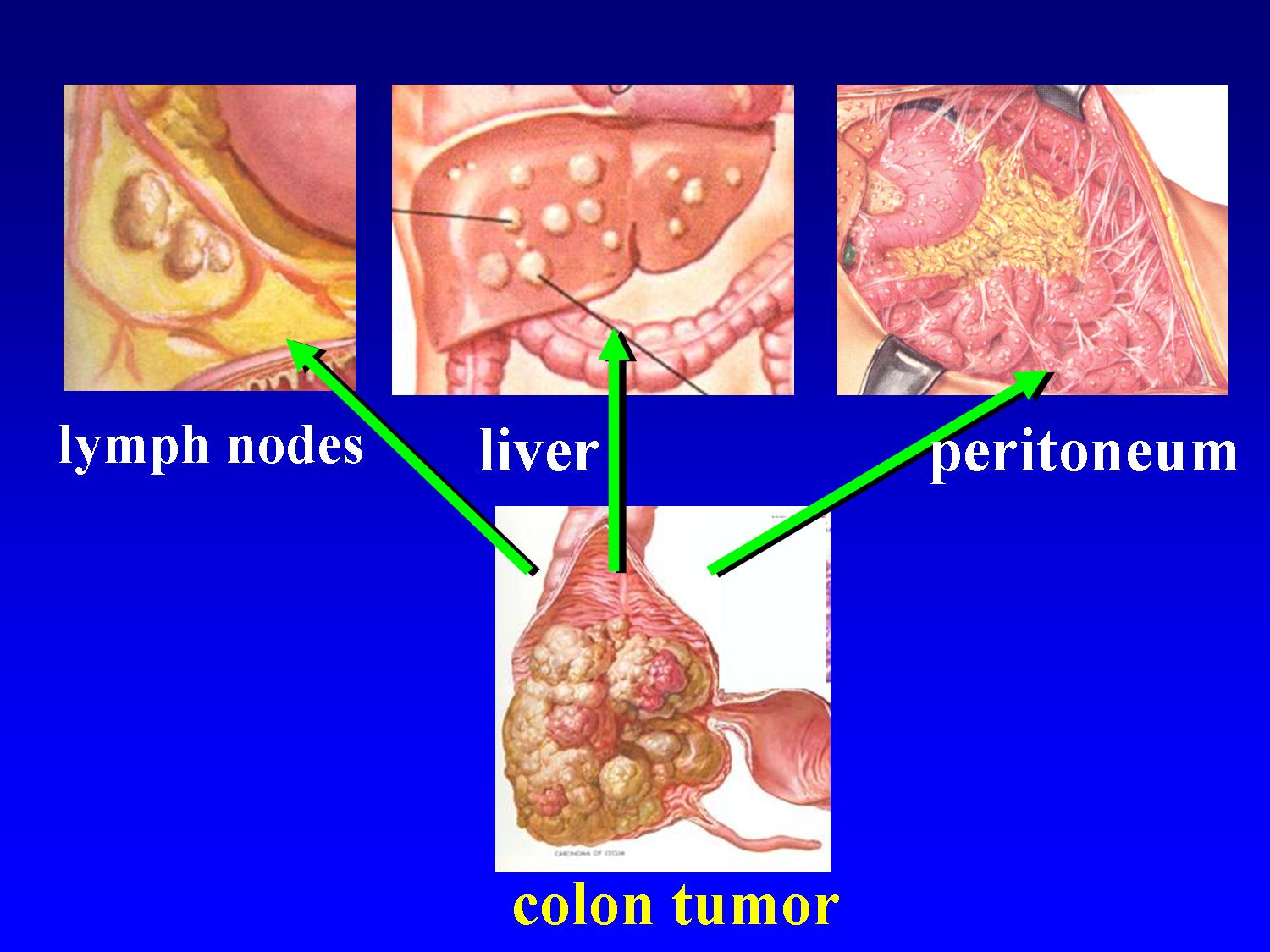
Tumors of the abdominal cavity, such as tumors of the large bowel (colon) and tumors of the ovaries can spread (seed) in three ways:
-via the lymphatic vessels to the lymph nodes
-via the blood vessels to other organs such as to the liver or the lungs
-via the abdominal cavity to the peritoneum
Patients with peritoneal implants often have seeding in the liver or lungs. In some patients however, seeding is limited to the peritoneum. It is for this subgroup of patients that a HIPEC may be an option.
What are the consequences of peritoneal cancer?
Peritoneal cancer can lead tot two types of complaints:
-Formation of ascites (accumulation of fluid in the abdominal cavity). In every healthy person, a small amount of fluid is present in the abdominal cavity, to facilitate the smooth gliding of the small bowel. This fluid is being produced continuously, especially by the peritoneum of the small bowel, and is being absorbed continuously as well, especially by the peritoneum of the underside of the diaphragm (respiratory muscle between the thoracic cavity and the abdominal cavity) and by the peritoneum of the omentum (an ‘apron’ of fatty tissue which is attached to the stomach and which lies over the small bowel). In peritoneal cancer, there can be an imbalance between production and absorption of fluid, e.g. by blocking of the absorption by the tumor implants, resulting in ascites. The patient notices that he or she is rapidly gaining weight and that the abdomen is swelling.
-Bowel obstruction. The tumor implants can cause the small bowel to stick to itself and to the abdominal wall, reducing mobility of the bowel and causing sharp angles. The tumor implants at the outside of the bowel can compress the bowel by their volume and block the passage of the bowel contents. This results in abdominal cramps, vomiting, absent passage of gas and stools, and a swollen abdomen.
What are the most frequent causes of peritoneal cancer?
In colon cancer (cancer of the large bowel), peritoneal cancer will develop in about 15% of the patients. Patients with peritoneal implants often have seeding in the liver or lungs. In 3% of all patients however, seeding is limited to the peritoneum. It is for this subgroup of patients that a HIPEC may be an option (see below).
In ovarian cancer (cancer of the ovaries), peritoneal cancer will develop in about 75% of the patients. In 50% of all patients, seeding is limited to the peritoneum. It is also for this subgroup of patients that a HIPEC may be an option (see below).
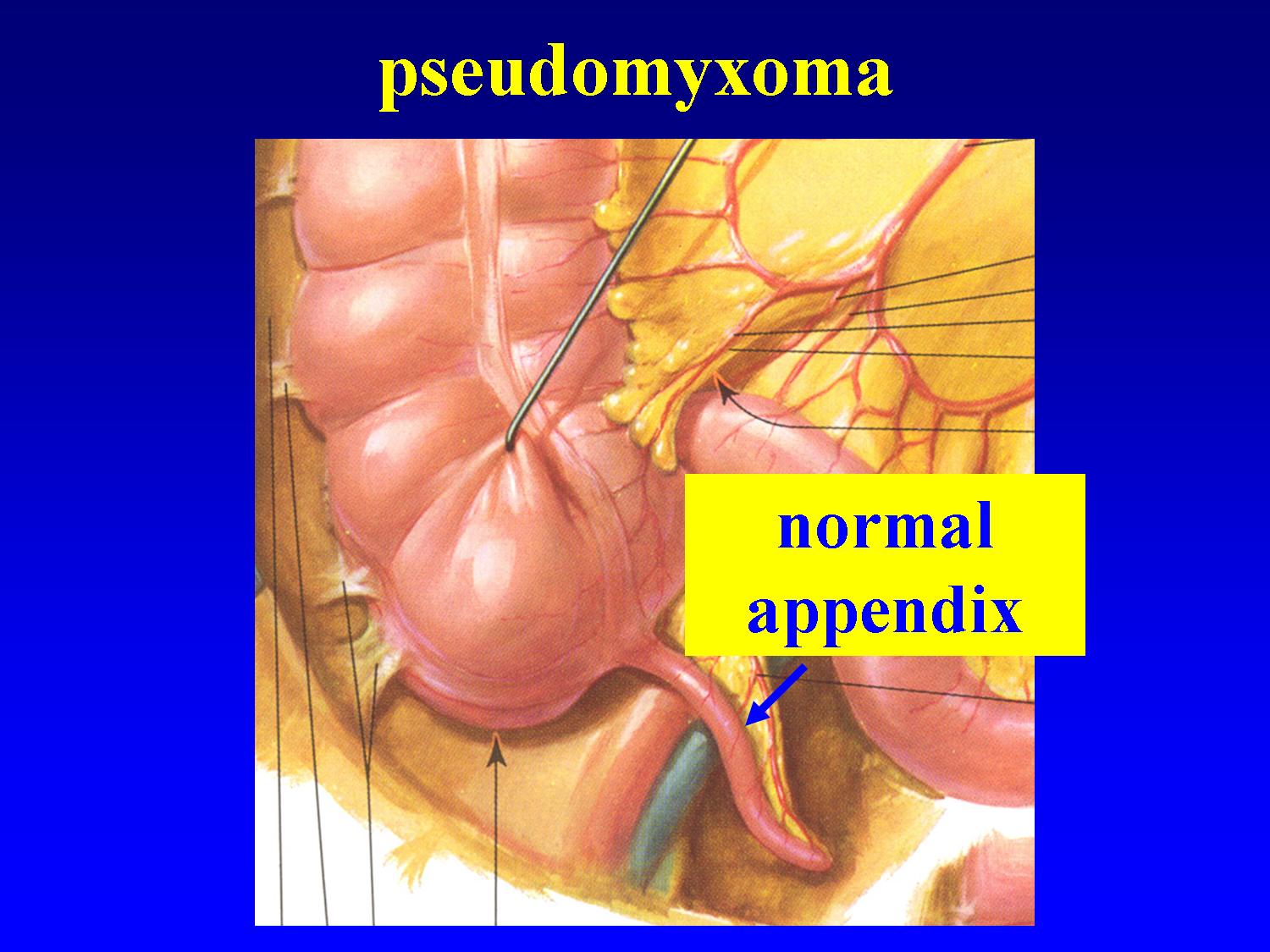
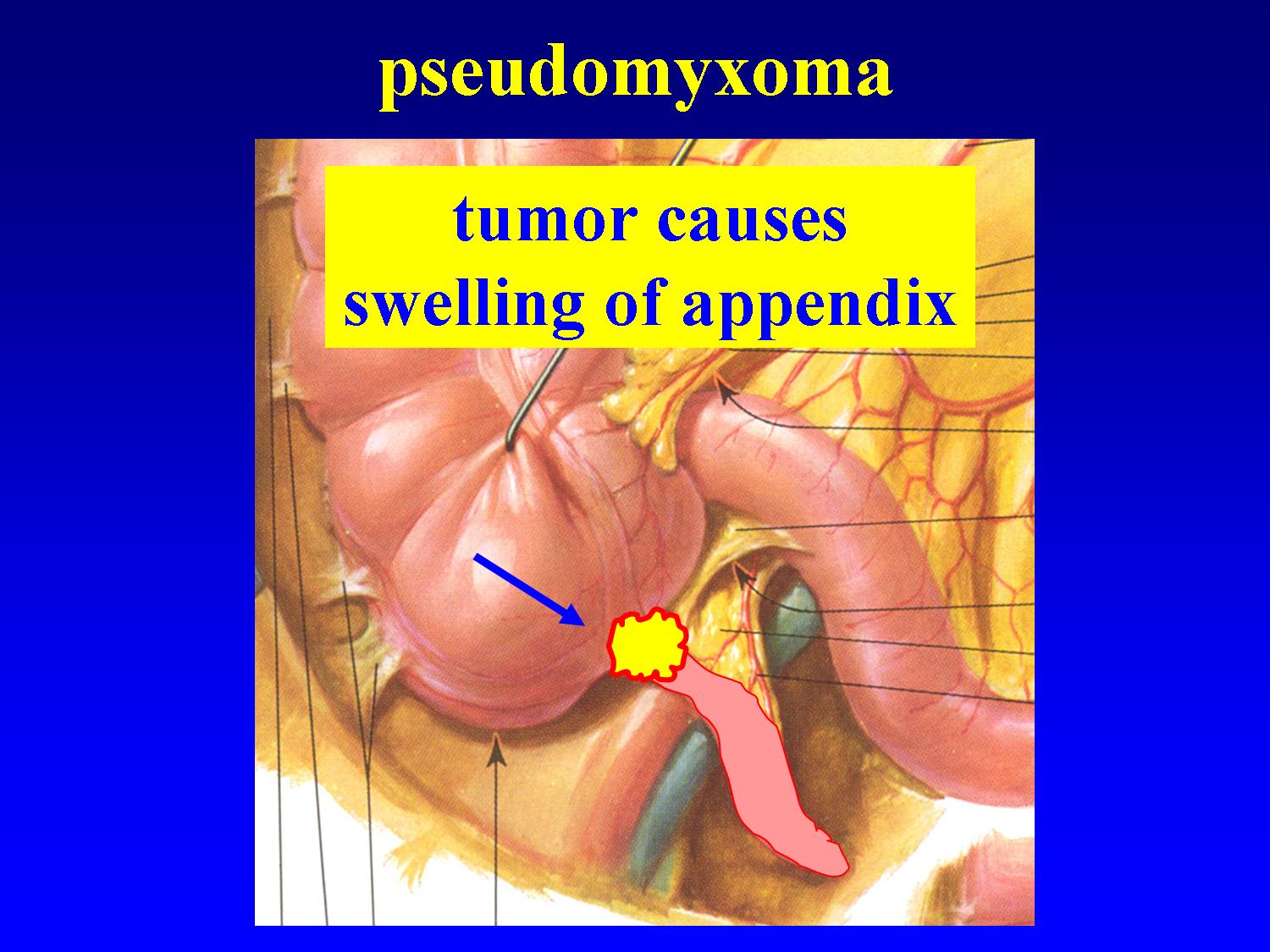
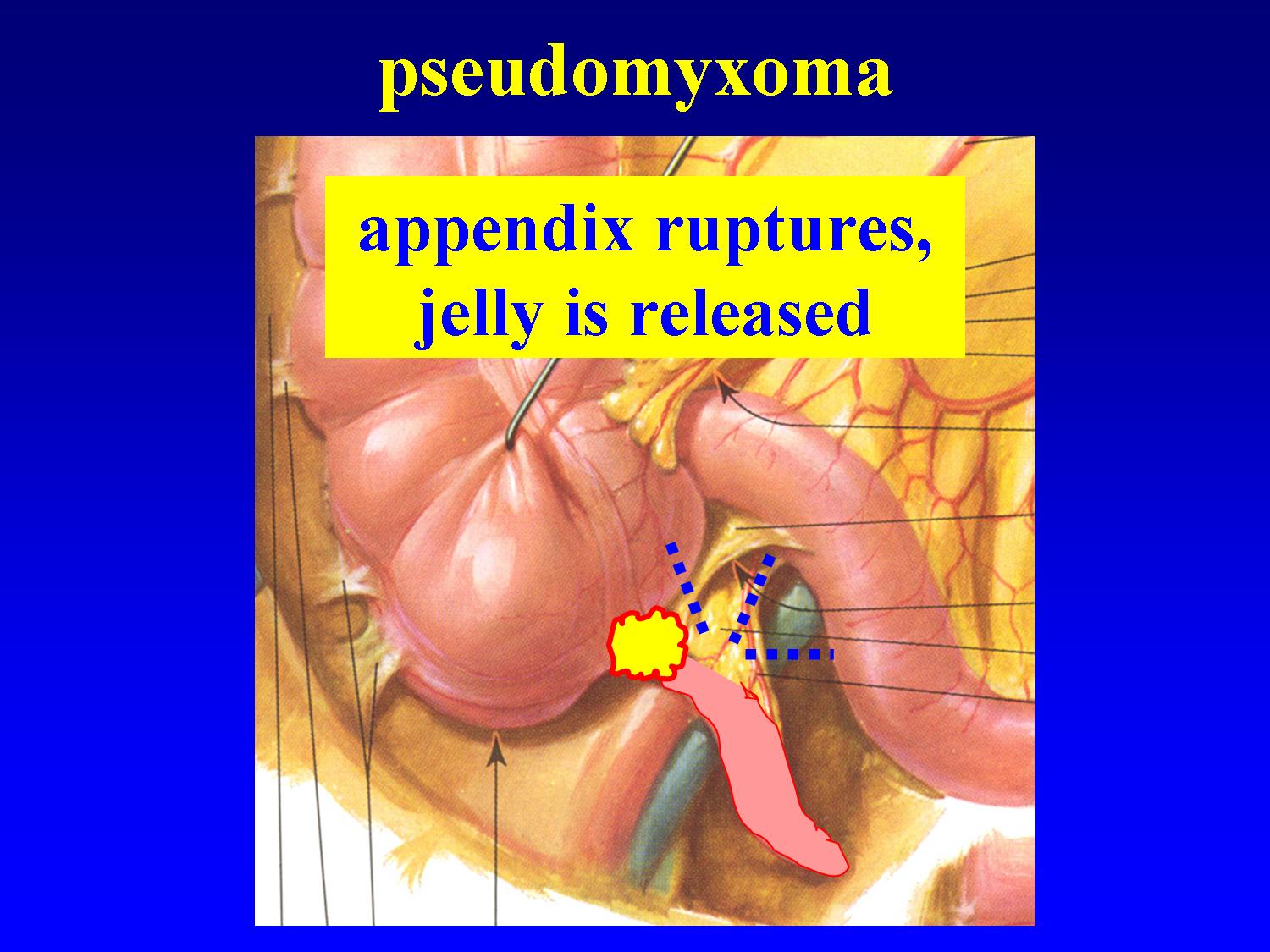
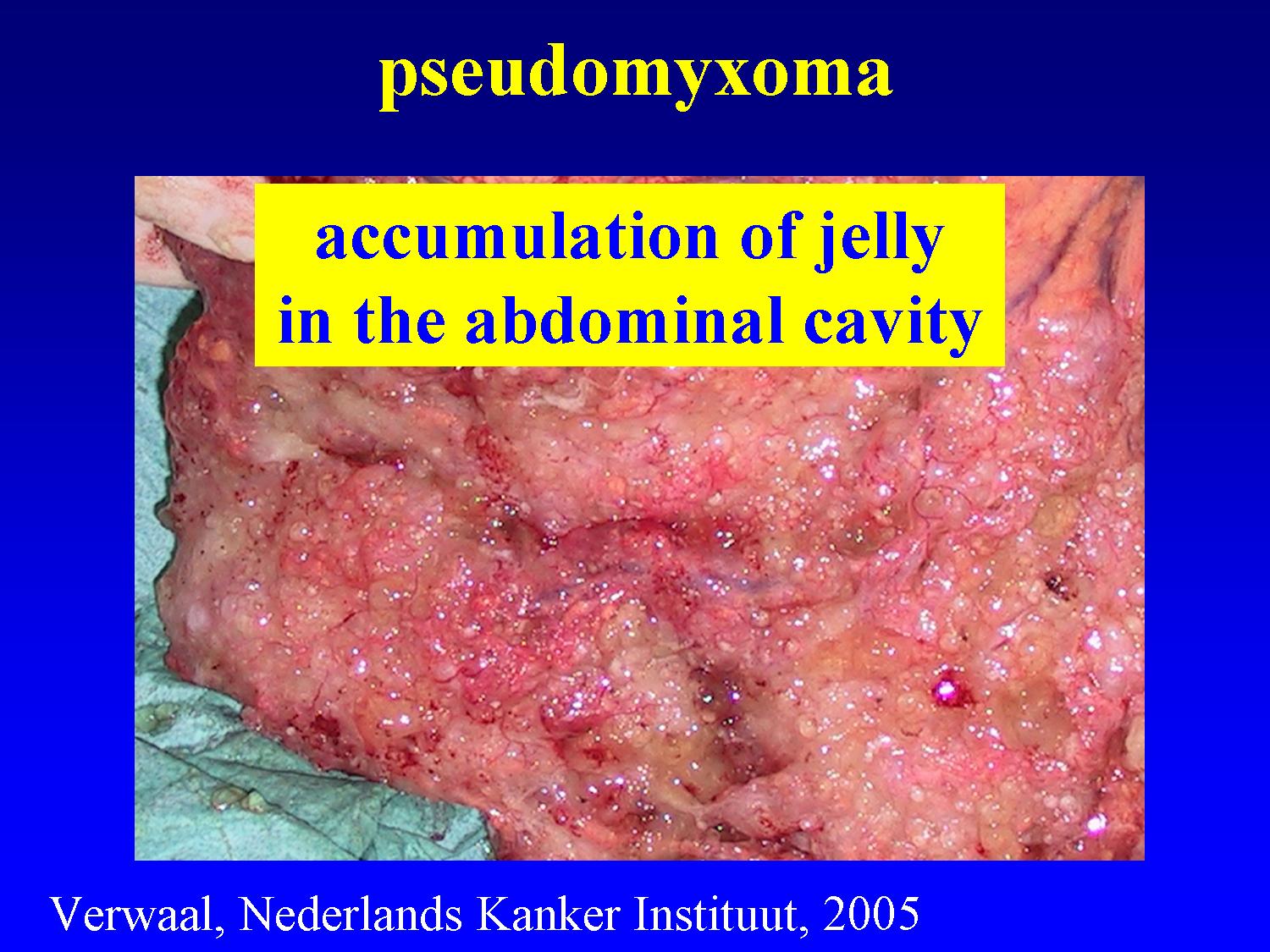
A pseudomyxoma is a rare form of peritoneal cancer. At its origin is a rather benign small tumor at the base of the appendix which blocks the passage. Jelly accumulates in the appendix which eventually bursts, releasing jelly and tumor cells in the abdominal cavity. These tumor cells continue to produce jelly, which results in a swollen abdomen and sticking together of parts of the small bowel with obstruction (see before). A HIPEC is regarded in many centers as the first choice treatment of this slowly growing tumor.
A mesothelioma is also a rare form of peritoneal cancer which begins in the cells of the peritoneum itself. In a first, more benign, type of mesothelioma, there is much ascites (peritoneal fluid) and only small tumor implants. In a second, more malignant, type of mesothelioma, there is little ascites but larger tumor implants. A HIPEC can be an option, especially for the first type.
Peritoneal seedings are frequent in stomach cancer. In Japan, HIPEC is being used as a preventive measure in advance stomach cancer, apparently with good results. Stomach cancer in Japan and stomach cancer in the West however cannot be compared directly. There are no good scientific data yet on the value of HIPEC in stomach cancer in the West.
Finally, peritoneal cancer can be caused by a lot of tumors inside or outside the abdominal cavity such as pancreas cancer, biliary cancer, sarcoma (cancer of the connective tissue) and breast cancer. At present, there are no scientific data to support the use of HIPEC in these settings.
What was the classical treatment of peritoneal cancer?
Until recently, the classical treatment of peritoneal cancer consisted of intravenous chemotherapy. In case of obstruction, a surgical intervention, such as a bypass between the bowel segment before and the segment behind the obstruction, was often carried out. In case of ascites (peritoneal fluid), medication to expulse fluid was prescribed and punctions were performed if necessary.
What has changed recently in the treatment of peritoneal cancer?
Since about twenty years, Professor Paul Sugarbaker applies the HIPEC treatment in patients with peritoneal cancer in the United States (see below). This surgical intervention appeared to give good results but did not gain acceptance by surgeons outside the center of Professor Sugarbaker because of the absence of comparative studies between patients who underwent the operation and patients who didn’t.
This changed with the publication of the Netherlands Cancer Institute of Amsterdam in September 2003 of the first and up till now only comparative study in patients with peritoneal cancer by a colon tumor (bowel cancer). For the first time, this study showed that patients who underwent a HIPEC fared better than patients with a classical treatment (see above). Some patients appeared to be cured (or at least to obtain a long survival), which is not possible up till now with chemotherapy alone. All patients taken together, including those who eventually died, there was a mean survival benefit of one year.
Since this study, several oncological centers in Europe and the United States have started performing HIPEC treatments with several variants. Stefaan Mulier, M.D., who is working now in the Leopold Park Clinic in Brussels, Belgium, is applying the original technique of the Netherlands Cancer Institute of Amsterdam since 2001.
What is a HIPEC?
HIPEC stands for: Hyperthermic IntraPEritoneal Chemotherapy, which means: rinsing of the abdominal cavity with heated chemotherapy. This surgical treatment consists of three different phases: exploration, debulking and chemotherapy itself.
1. exploration
The surgeon opens the abdomen with a long incision at the midline. After liberating adhesions, he will carefully evaluate the peritoneal cancer. He will look for an answer to three questions:
1. What is the extension of the peritoneal cancer?
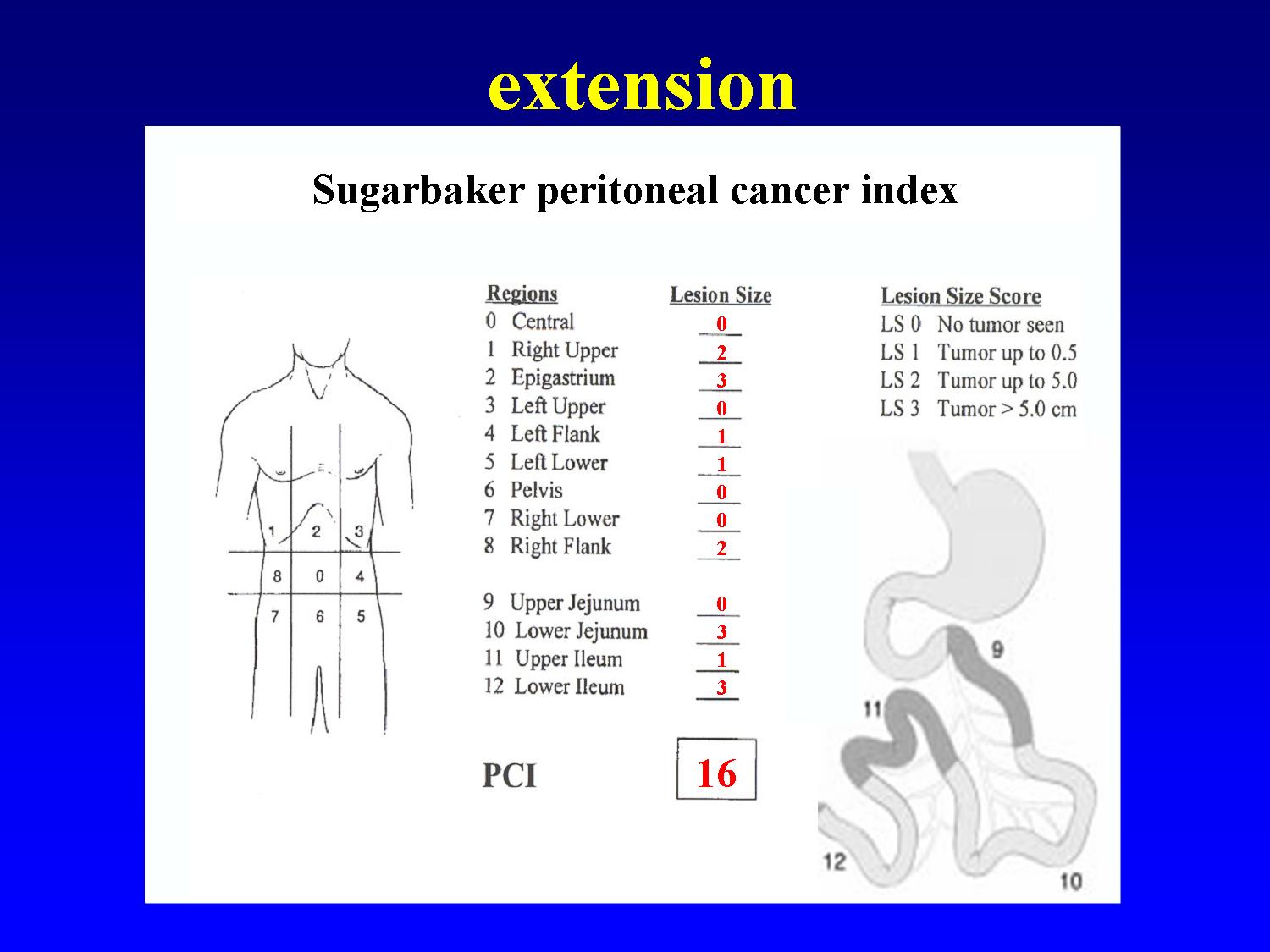
The surgeon measures the amount of cancer in 13 different regions of the abdomen and gives each region a score from 1 to 3. These scores are added to a global score (Sugarbaker Peritoneal Cancer Index). This scoring has a double aim. In case of peritoneal cancer by a bowel tumor, it allows to avoid a meaningless operation: when the score is higher than 20, the chances of improving survival by performing a HIPEC are very small and the intervention is stopped. In addition, the score allows an estimation of the prognosis. The lower the score, the better the prospects.
2. Can all tumor implants be removed?
Especially in case of peritoneal cancer by a bowel tumor, it is very important to remove all visible tumor implants before rinsing the abdomen with the heated chemotherapy. When not all visible tumors can be removed, the chances of improving survival by performing a HIPEC are very small and the intervention is stopped. This can be the case when a too large part of the small bowel is covered with tumor: to allow normal food absorption, at least 1.5 m (of about 3 m) small bowel must remain after resection. Secondly, the vessels to the liver can be encased by tumor at the site where they enter the liver, rendering impossible a complete tumor clearance. Thirdly, part of the stomach can be covered by tumor. Although partial or total resection of the stomach is technically possible, quality of life after HIPEC with stomach resection is too poor due to difficult food intake to justify a HIPEC in these cases.
3. Are there seedings in the liver?
Despite all progress in imaging techniques that are done before an operation (CT scan, magnetic resonance imaging, PET scan), it is not possible to exclude with a 100% certainty seedings in the liver (liver metastases). Therefore, the surgeon carries out a liver ultrasound during the operation. In case of liver seedings, the chances of improving survival by performing a HIPEC are very small and the intervention is stopped.
When the peritoneal cancer is not too extensive, appears to be completely resectable, and is not accompanied by liver metastases, the surgeon proceeds with the debulking. If not, a HIPEC is not carried out and the risk of obstruction is evaluated. In case of imminent obstruction, a bypass between the bowel segment before and the segment behind the obstruction is realised.
2. debulking
Debulking or cytoreduction means surgical removal of all visible tumor implants.
-the peritoneum at the sites of the tumor implants.
-the omentum; an apron of blood vessels and fatty tissue which is attached to the stomach, covers the small bowel, and is often loaded with tumor (forming an ‘omental cake’.
-according to the situation of the individual patient, removal of the spleen, of the gallbladder, of the uterus and ovaries, of part of the diaphragm, of part of the small or the large bowel or of other organs may be required.
It is mainly this part of the intervention which can last many hours.
3. rinsing of the abdominal cavity with heated chemotherapy
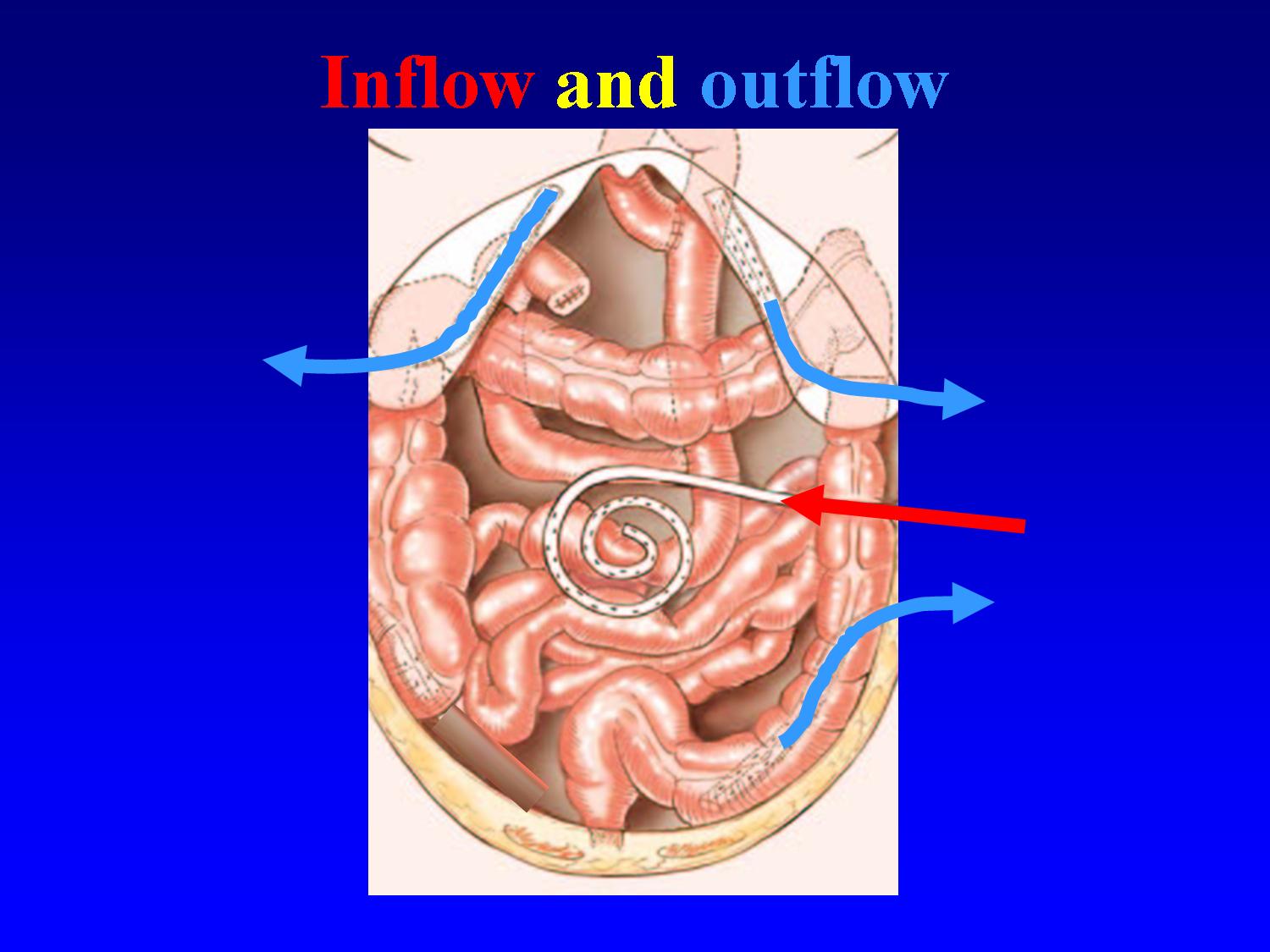
After all visible tumor has been removed, the abdominal cavity is rinsed with heated chemotherapy. Tubes are applied in the abdominal cavity to bring heated fluid from a reservoir to the abdomen and to aspirate it again in a closed circuit. As soon as the desired temperature has been reached, the chemotherapy is being added to the fluid. In a common treatment protocol for colon cancer, Mitomycine C is used at 41.5° Celsius during 90 minutes. For other tumors, other protocols are being used.
What is the aim of rinsing the abdominal cavity with heated chemotherapy?
The rinsing of the abdominal cavity with heated chemotherapy aims to kill the microscopic tumor implants, that are invisible to the naked eye, and that remain after removal of the visible tumor.
Chemotherapy which has been poured into the abdominal cavity hardly leaves the abdomen, causing much less secondary effects to the rest of the body than the same dose of chemotherapy given intravenously. This way, a much higher amount of chemotherapy can be given, exposing tumor cells to drug concentrations that are up to 100 times higher than for intravenous chemotherapy.
Furthermore, by heating this chemotherapy to temperatures between 41-43° Celsius, the tumor-killing effect is increased as well as the depth of penetration into the small tumor remnants.
What is the duration of hospitalisation?
After the intervention, the patient stays about three days in the intensive care unit before going to the surgical ward. It usually lasts about two weeks before the patient can eat normally. The evacuation of the stomach is being disturbed for some time after a HIPEC. Food is being administered temporarily with a feeding tube directly into the small bowel, which regains its normal function more rapidly than the stomach. Total hospitalisation lasts about 2 to 4 weeks. Its duration is determined mainly by the time of restoration of normal stomach evacuation.
What happens after the patient returns home?
During hospitalisation and after returning home, the patient receives physical revalidation therapy for several weeks, which has a positive influence on recovery after this heavy operation. The patient is frequently seen at the outpatient clinic to monitor recovery, to progressively adapt the diet, to answer questions, and to offer a psychological support.
When the patient has recovered sufficiently both physically and psychologically after the intervention, generally an intravenous chemotherapy is given for 6 months.
Follow-up examinations (tumor marker, CT scan) are planned on a regular basis.
What kind of secondary effects can occur?
A HIPEC is a rather heavy operation which requires a lot of physical and psychological energy from the patient. A lot of patients feel very tired during about three months. Appetite can be lowered in this period. Moments of dejectedness are not unusual. A high prior motivation, correct information, and a good support by the family, the surgeon, the general practitioner, the diet consultant and the physiotherapy consultant are of major importance. After three months, quality of life returns to the level prior to the operation.
What kind of complications can occur?
After a HIPEC, complications occur in about 30% of patients.
-Complications that are possible after any surgical intervention, such as infection or bleeding, can occur after a HIPEC too.
-Some complications are more specific to a HIPEC:
°An increased risk of leakage of bowel junctions (anastomoses) due to the heated chemotherapy. In case of increased risk of leakage, the surgeon can judge that it is safer to temporarily create a stoma (the bowel is exteriorized through the abdominal wall).
°fluid accumulation in the pleural cavity (the space between the lungs and the thoracic cage), especially when tumor was removed from the diaphragm. In case of tumor at the diaphragm, the surgeon will put a tube (thoracic drain) in the thorax as a preventive measure to drain any fluid after the operation for some days.
°slow emptying of the stomach for about two weeks (see above)
-Complications of the chemotherapy itself (lowering of white blood cell count, lowering of platelet count) can occur after a HIPEC, depending on the drug and the dose that is used, but are usually rare.
Is a HIPEC worth all the effort?
A HIPEC is a rather heavy operation, with a hospitalisation of some weeks and a certain risk of complications. Does sufficient scientific proof exist at present that a HIPEC improves survival over a classical treatment?
colon cancer (cancer of the large bowel)
In September 2003, the first and up till now only good comparative study (technical term: randomized study) in patients with peritoneal cancer by a colon tumor was published. For the first time, this study showed that patients who underwent a HIPEC fared better than patients with a classical treatment. Some patients appeared to be cured (or at least to obtain a long survival), which is not possible up till now with chemotherapy alone. All patients taken together, including those who eventually died, there was a mean survival benefit of one year.
ovarian cancer
In peritoneal cancer by an ovarian tumor three good comparative studies (technical term: randomized studies) have been published. Each of these studies has shown that survival is better after adding intraperitoneal chemotherapy to the classical treatment of debulking and intravenous chemotherapy. The intraperitoneal chemotherapy in these studies however was different from a HIPEC as described above in two ways: the rinsing of the abdomen with chemotherapy was not realised during the debulking operation but for some days to weeks after the operation by means of tubes that were left in the abdomen. Furthermore, the chemotherapy solution was not heated. Despite this theoretically suboptimal administration of the intraperitoneal chemotherapy, a clear benefit of this technique has been demonstrated.
In addition, one comparative study has compared a 'real' HIPEC to standard treatment. It showed that survival was much better after a HIPEC. This study however, by its design, had less scientific 'convincing' power than the above mentioned studies (technical term: retrospective study).
In conclusion, there are hopeful indications, but not yet final proof by a scientifically optimal study (technical term: randomized study) to state that a HIPEC is useful in peritoneal cancer of ovarian origin. At the Leopold Park Clinic in Brussels we take part in an international study to determine with more scientific certainty whether this is the case or not.
pseudomyxoma
This type of slowly growing peritoneal cancer is rare (see above). It causes an accumulation of jelly in the abdominal cavity with only few tumor cells. In the past, treatment consisted of repeated surgical interventions with aspiration of all jelly. Many centers currently apply a HIPEC. Survival is often prolonged thanks to the slow growth rate of the tumor. Whether the results of a HIPEC are better than the classical treatment cannot be determined at present with scientific certainty because there are no comparative studies due to the rarity of this tumor. Despite this lack of sound evidence, many centers recommend a HIPEC as the first choice treatment for a pseudomyxoma.
mesothelioma (cancer of the peritoneum itself)
A mesothelioma is also a rare form of peritoneal cancer. In a first, more benign, type of mesothelioma, there is much ascites (peritoneal fluid) and only small tumor implants. In a second, more malignant, type of mesothelioma, there is little ascites but larger tumor implants. A HIPEC can be an option, especially for the first type. It often makes the invalidating ascites to disappear. Due to the rarity of this tumor there are no comparative studies to prove the benefit of a HIPEC. Despite this lack of evidence, many centers recommend a HIPEC, especially for the first type.
Peritoneal seedings are frequent in stomach cancer. In Japan, HIPEC is being used as a preventive measure in advance stomach cancer, apparently with good results. Stomach cancer in Japan and stomach cancer in the West however cannot be compared directly. There are no good scientific data yet on the value of HIPEC in stomach cancer in the West. Scientific research has shown however that a HIPEC does not improve survival when compared to a classical chemotherapy in the following cases:
-when a complete debulking is not possible
-when tumour nodules measure more than 5 mm
-when ascites is present
and therefore is not indicated in those cases.
Finally, peritoneal cancer can be caused by a lot of tumors inside or outside the abdominal cavity such as pancreas cancer, biliary cancer, sarcoma (cancer of the connective tissue) and breast cancer. At present, there are no scientific data to support the use of HIPEC in these settings.
In which patients a HIPEC can be indicated?
colon cancer (cancer of the large bowel)
The surgeon will evaluate carefully whether or not a HIPEC is indicated for each individual patient. The first part of this evaluation takes place before the operation, while the second part is performed during the operation. The final decision to proceed or not with a HIPEC is taken after the exploratory phase of the operation.
1. before the operation
-age: the patient should not be too old. An age of less than 70 year is a relative criterion. The younger the patient, the better the intervention is supported. Some patients who are just above the age of 70 year and who have limited peritoneal cancer and an excellent general condition can still be taken into account.
-high motivation: the patient must be prepared to ‘fight’ to support this rather heavy operation.
-chemotherapy options: there should remain some chemotherapy options for administration after the operation. When the peritoneal cancer has become resistant to all lines of chemotherapy, a HIPEC is not a good option.
-good general condition, absence of obstruction and absence of ascites. In case of poor general condition, obstruction or ascites, the results of a HIPEC are poor and the risk of complications is significantly higher. Please note that these criteria are valid only for peritoneal cancer due to colon cancer.
-absence of seedings to the liver of the lungs. In these cases it is unlikely that a HIPEC is better than a classical intravenous chemotherapy treatment.
2. during the operation (see above)
-extension (score of Sugarbaker)
-resectability
-seedings to the liver
When the Sugarbaker Peritoneal cancer Index is higher than 20, when not all visible tumor can be removed, or in case of seedings to the liver, the chances of improving survival by performing a HIPEC are very small and the intervention is stopped (see above).
ovarian cancer
The surgeon will evaluate carefully whether or not a HIPEC is indicated for each individual patient. The first part of this evaluation takes place before the operation, while the second part is performed during the operation. The final decision to proceed or not with a HIPEC is taken after the exploratory phase of the operation.
1. before the operation
-age: the patient should not be too old. An age of less than 70 year is a relative criterion. The younger the patient, the better the intervention is supported. Some patients who are just above the age of 70 year and who have limited peritoneal cancer and an excellent general condition can still be taken into account.
-good general condition
-high motivation: the patient must be prepared to ‘fight’ to support this rather heavy operation.
-chemotherapy options: there should remain some chemotherapy options for administration after the operation. When the peritoneal cancer has become resistant to all lines of chemotherapy, a HIPEC is not a good option.
-absence of seedings to the liver of the lungs. In these cases it is unlikely that a HIPEC is better than a classical intravenous chemotherapy treatment.
2. during the operation
-resectability: after the intervention no tumor implants larger than 1 cm should remain
-seedings to the liver
When not all visible tumor larger than 1 cm can be removed, or in case of seedings to the liver, the chances of improving survival by performing a HIPEC are very small and the intervention is stopped (see above).
other tumors
For the other, rarer types of peritoneal cancer, similar criteria are being used.
Closing remark
The information on this page aims to provide general background information to patients with peritoneal cancer. This way, the patient can prepare the questions he wants to ask to the HIPEC surgeon, and he can read this text again after the visit to the surgeon. Each patient with his disease however is unique; and the surgical and medical treatment of peritoneal cancer is evolving rapidly so that the information by your doctor or the treatment he proposes may differ slightly from this introductory background information. The information given by your doctor however always ranks above the information on this page.
© This information is copyrighted